We need health professionals to raise the issue across the UK, to knock on the door of government to ask that the rest of this pandemic is managed using tried and tested health protection and outbreak control measures as it continues to decline.
The UK governments it would appear still seem to be in denial over mild symptoms that are associated with infection with COVID (SARS- CoV-19), continuing to maintain the line that to book a test via their portal (https://www.gov.uk/get-coronavirus-test) you can only do so if you have one of the COVID-3 i.e.:
- a high temperature
- a new, continuous cough
- you’ve lost your sense of smell or taste or it’s changed
There are other reasons why you are able to get a test but none are related to any of the known COVID symptoms other than the above (if you want to see my journey trough the questions, I recorded images on my device here: https://phw.org.uk/gov-uk-journey/)
Yet the UK government has now arrived at the conclusion that up to one third of people with the virus have no symptoms whatsoever, with a recent tweet stating, “Around one in three people with COVID19 do not have symptoms.” This official line has slowly increased with time. I suspect the world will settle eventually around the 50% mark given that in April 2020, the BMJ noted the rate in China was 80% and a previous University College London study, suggests up to 75%.
It must surely be inconceivable to any thinking person that there are only asymptomatic infections or infections associated with just fever, continuous cough or loss of smell or taste. As I discussed previously, I remain disturbed over this failure to manage this respiratory virus like any other in an outbreak and recognise that individuals present with a wide range of symptoms. There is plenty of discussions of the wider COVID symptoms:
The COVID Symptom Study (Zoe App) December 7th 2020 reported the wide range of symptoms being seen in the UK.
The Office for National Statistics in their January 2021 report lists percentages positive for the following prompted symptoms in the UK:
- Abdominal pain
- Cough
- Diarrhoea
- Fatigue weakness
- Fever
- Headache
- Loss of smell
- Loss of taste
- Muscle ache myalgia
- Nausea vomiting
- Shortness of breath
- Sore throat
Similarly, Imperial College (London) in a recent pre-print (awaiting peer review) lists details of the wide range of symptoms, again based on their UK study.
With others across the world now moving to focus on these wider range of symptoms:
You can see how New South Wales, Australia advise testing for a wide range of symptoms – bear in mind, Australia and New Zealand have been praised for their approach.
The USA Communicable Disease Centre also advise testing for a wide range of symptoms
Similarly, the World Health Organisation list a wide range of symptoms that should prompt testing, albeit they refer to these milder symptoms as, “less common” but that may be a reflection of the earlier testing like in the UK that emphasises the COVID-3 and therefore created a selection bias of the symptoms. The ONS survey and the Imperial College paper above, both use a structured approach to establish the true underlying likelihood of a range of symptoms.
I am of course, pleased my own health board, together with Swansea Bay University Health Board are offering testing to individuals with wider symptoms.
I’m trusting at some point soon, even those at the top of government who seem determined to maintain this COVID-3 mantra, will see sense and move to testing for the wider range of symptoms and focus less on asymptomatic testing, with tests that I have explained previously are not suitable for screening because of their poor sensitivity.
As the incidence of disease across the country declines, if we do not change our focus from asymptomatic testing to wide symptomatic testing, we will put patients at risk, albeit the numbers at risk should also decline as the incidence declines. But if that leads to a number of unnecessary deaths, it will be of no comfort to their grieving families.
One of my colleagues answered a question on the use of Lateral Flow Devices and their ability to detect asymptomatic cases of COVID (https://www.facebook.com/PublicHealthWales/videos/318867956235876)
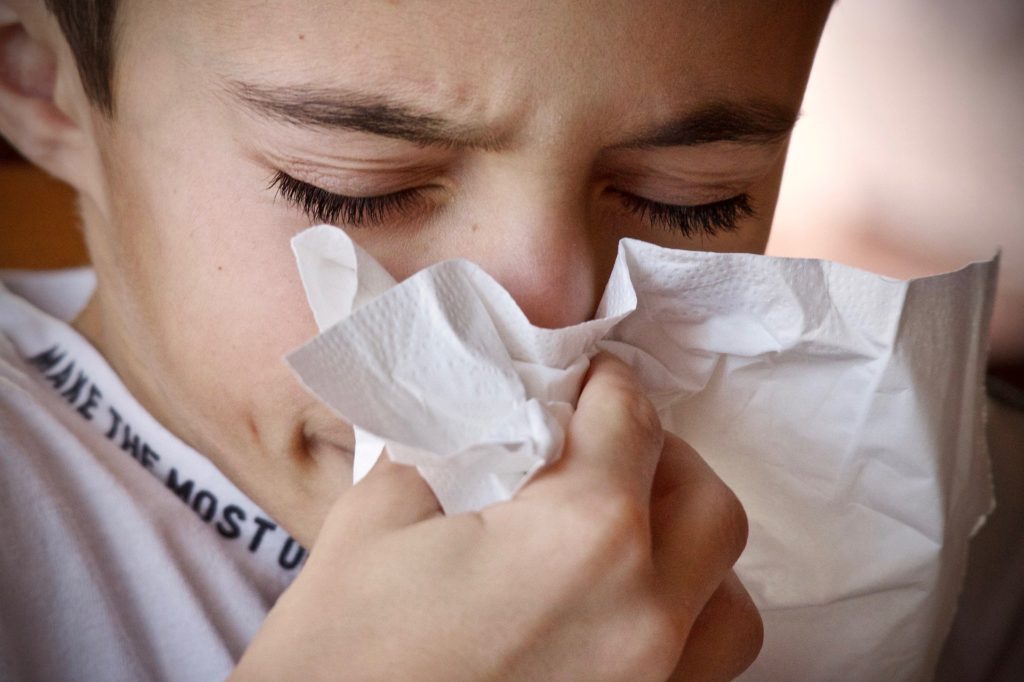
As he explains, the sensitivity of these tests when used for mass screening programmes in the likes or Liverpool in England and Merthyr Tydfil in Wales achieved a sensitivity of around 50%. He does not quote the specificity but that is reported to be around 99.90% compared with that for the PCR test of 99.96%.
Public Health Wales reports the figures daily and you can find the generally twice weekly report for the 7-day incidence by county by clicking the tab at the top of the screen labelled, “Local Authorities table” and scrolling to the bottom of the page to click the link on the left labelled “Download Report.” The figure for my part of Wales, Hywel Dda University Health Board (Carmarthenshire, Ceredigion and Pembrokeshire) was 34.3/100,000 (with the mean for Wales 52.6/100,000), although that was for the period to 27th February and it has reduced further since. Using these figures, this is the effect:
In other words, if we test 100 people, they will all be negative. If we test 1,000 people, we will get one positive but it is a false positive. When we test 10,000 people, we get 12 positives but only 2 are true positives, ten are false positives and we will miss 2 people with the infection as they will give us a false negative test. Now the effect in the workplace is not that dramatic but if you have 500 employees testing twice weekly (1,000 tests), someone will test positive every week, will have to not work until they have got a PCR test to demonstrate they are a false positive. Ten weeks in and you will have sent 12 people off work, brought 10 back perhaps the next day and 2 will be self isolating for 10 days. Will you have stopped the spread in the workplace? Who knows but there will still be 2 people during that period at work with the virus.
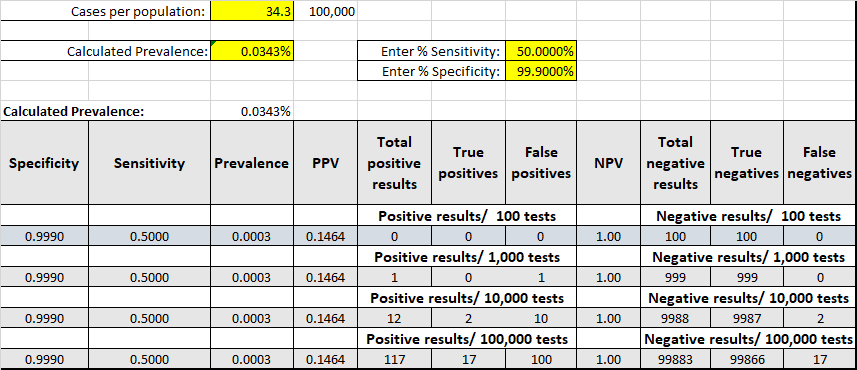
My colleague in the video above advised that people who are doing this regularly get better at testing and improve the sensitivity to that same as that of practiced healthcare workers doing the original PCR tests i.e. around 70%:
You still have the same 10 false positives but the improved sensitivity means the false negatives are reduced to 1. You will also still have the same 10 false positives, having at least a day off work while they get their PCR test.
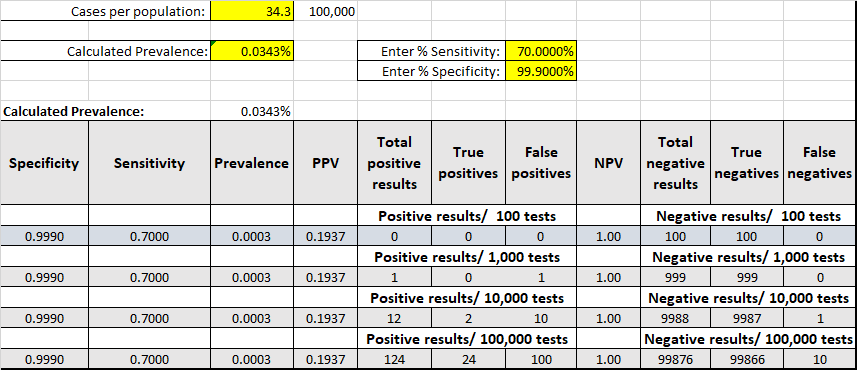
If instead of screening different populations, we were to investigate all the people with minor respiratory symptoms, we improve the diagnostic yield because these are the people who are more likely to have the virus. What we are doing is selecting those people who are more likely to be positive. In such a subgroup we can see what happens to the figures. Here’s the effect if in the group with respiratory symptoms, 10% have COVID:
Now we become a much more efficient testing machine. We start picking up the positives more quickly because we have honed in on the people most likely to have the virus and for every 100 people we now test in this group, we find 7 of the 10 with the virus. We still see approximately the same number of false positives, 9 rather than 10 when testing 10,000 but we will be feeling much better about the effectiveness of the testing regime because in that selected group, we have now found 700 infected people.
The Public Health Wales weekly influenza report has a link at the top of the page to allow you to see the most recent viral activity. Figure 3 on this report looks at surveillance testing for the GP sentinel testing across Wales. Although the activity is declining, you will see over the period of the recent COVID spike in cases, that the other virus circulating has primarily been the rhinovirus. If you look at week 44, you can see that of the people with symptoms tested, about a third were COVID, a third rhinovirus and the other third negative. This shows that our GP’s are expert at diagnosing respiratory viral infections, being correct on 2/3 of occasions.
This is a reflection of the clinical process. The GP assessment is if you like the first test in making a diagnosis. They will equally have a false positive and false negative rate but are the first stage of the assessment process. Based on their assessment, they would then determine what would help confirm the diagnosis. With the surveillance scheme, GP’s who are in practices that contribute, arrange for samples to be sent one everyone who fits the clinical criteria for a probable viral respiratory infection. They seem to be correct 2 times out of every 3 diagnoses, with in week 44, a third of the samples submitted were COVID positive. So if we therefore increase our diagnostic pre-test probability to 1/3 and say the incidence in our selected group is now 33%, i.e. 33,333/100,000 then this is the effect:
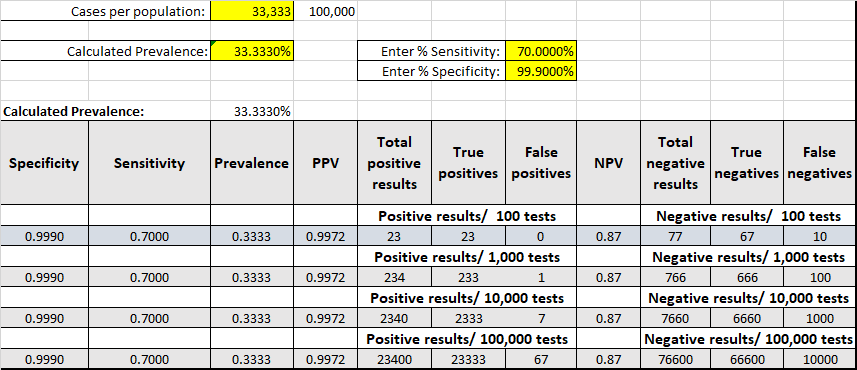
What this shows is a diagnostic test is a useful additional way of confirming a clinical diagnosis. It still is associated with false negatives but as the physician works towards a diagnosis, so different elements will be reconsidered, ever refining the final diagnosis. They cannot be used for screening. To be effective, a screening test must have a very high sensitivity, as close to 100% as possible, the aim being to detect all cases. The specificity is less important as other tests will then be used to find the true positives. Perhaps one of the best examples are the bowel screening programmes. The faecal tests for blood have a very high sensitivity but are not specific. Positive individuals undergo an endoscopy to look in the bowel directly for a cancerous growth and rule out the false positives.
Why is government ignoring testing the vast majority of people with symptoms?
This is something that we have not had an answer for so far and needs to continue to be raised. In Wales, there has been an emphasis on Value Based Healthcare and Prudent Healthcare.
The Bevan Commission, which “provides independent, authoritative advice on health and care to the Welsh Government and leaders in NHS Wales, the UK and beyond,” has a series of commentaries related to the COVID-19 pandemic. At the heart of the Bevan Commissions work is the concept of prudent healthcare. Principle 3 advises, “Do only what is needed – no more, no less – and do no harm.” For a concept at the heart of healthcare in Wales, I suggest the current testing strategy is very far from prudent. I suggest we Tweet @BevanCommission to suggest as part of their COVID-19 focus to consider whether this focus on testing meets their Prudent Healthcare principles.
The UK National Screening Committee (UK NSC), “advises ministers and the NHS in the 4 UK countries about all aspects of population screening and supports implementation of screening programmes,” yet surprisingly they do not appear to have been asked to review what is probably the biggest and most expensive screening programme the UK has mounted. Again, I suggest as professionals and public we Tweet them @PHE_Screening to seek their views on a screening programme utilising a diagnostic test with a sensitivity of less than 70%.
Please join me in asking for a redirection towards testing people with the wisest set of symptoms, rather than the current focus on the asymptomatic.
Update 16th March
CMO Wales has written to GP practices today (16th March) to advise of a change introduced by Public Health England, which advises a change to the testing regime to allow wider testing of symptomatic patients across GP practices (published 12th March). The letter announces that GP’s may now direct their patients to the portal, stating “From the 5th March, an additional criteria has been added to the online government booking portal for ordering a PCR test in order to enable GPs and health professionals to instruct someone to book a test on the online system if they feel it is required, no matter what their symptoms are.” The key for me here being, “No matter what their symptoms are.”
This is not quite the same as widening the symptom list on the opening screens of the portal but may be the first chink in the armour to move on the position.
Very interesting reading-thank you Mike! I would be very interested in hearing your thoughts on the following:https://www.nature.com/articles/s41467-021-22036-z (Exposure to SARS-CoV-2 generates T-cell memory in the absence of a detectable viral infection)
Eva, my apologies for the late approval and failure to respond earlier. I must have missed an email notification.
The findings in the paper are not perhaps that surprising. We know that even with someone who has some the cardinal 3 symptoms and severe disease, we may indeed see negative PCR tests but that other markers subsequently confirm exposure. This was previously reported with patients who had negative PCR tests then demonstrating an antibody response. So not surprising to see a similar finding now with cellular immunity.
Thank you Mike!